
Page 37 - TERMINAL DISCHARGE GUIDELINE FIRST EDITION 2023
P. 37
Chapter 7
Terminal Discharge Pathway
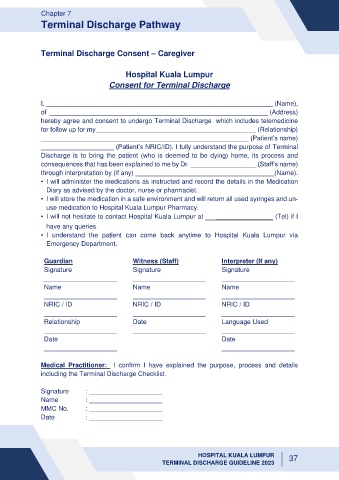
Terminal Discharge Consent – Caregiver
Hospital Kuala Lumpur
Consent for Terminal Discharge
I, (Name),
of (Address)
hereby agree and consent to undergo Terminal Discharge which includes telemedicine
for follow up for my____________________________________________ (Relationship)
_________________________________________________________ (Patient’s name)
____________________ (Patient’s NRIC/ID). I fully understand the purpose of Terminal
Discharge is to bring the patient (who is deemed to be dying) home, its process and
consequences that has been explained to me by Dr. __________________ (Staff’s name)
through interpretation by (if any) (Name).
• I will administer the medications as instructed and record the details in the Medication
Diary as advised by the doctor, nurse or pharmacist.
• I will store the medication in a safe environment and will return all used syringes and un-
use medication to Hospital Kuala Lumpur Pharmacy.
• I will not hesitate to contact Hospital Kuala Lumpur at _____________________ (Tel) if I
have any queries.
• I understand the patient can come back anytime to Hospital Kuala Lumpur via
Emergency Department.
Guardian Witness (Staff) Interpreter (If any)
Signature Signature Signature
____________________ ____________________ ____________________
Name Name Name
____________________ ____________________ ____________________
NRIC / ID NRIC / ID NRIC / ID
____________________ ____________________ ____________________
Relationship Date Language Used
____________________ ____________________ ____________________
Date Date
____________________ ____________________
Medical Practitioner: I confirm I have explained the purpose, process and details
including the Terminal Discharge Checklist.
Signature : ____________________
Name : ____________________
MMC No. : ____________________
Date : ____________________
HOSPITAL KUALA LUMPUR 37
TERMINAL DISCHARGE GUIDELINE 2023